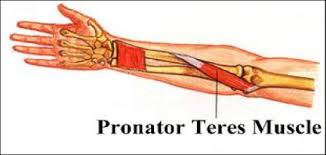
The Pronator Syndrome is a painful condition of the forearm and hand. It is caused by compression of the median nerve by the pronator teres muscle. The pain is located in the forearm and radiates to the first three and half fingers of the hand. It may radiate proximally as well into the elbow. It is made worse may repetitive motions. It is most common in middle aged females but also occurs in men whose job includes these repetitive motions. It has similar symptoms both to both tennis elbow and carpal tunnel syndrome and can be easily mistaken for either one. Testing includes X-rays and MRIs of the forearm to exclude other causes such as fractures and tumors. Electromyography and Nerve Conduction studies are useful to determine the site of the nerve injury and to look for other coexisting problems such as a herniated cervical disc. Treatment begins with conservative modalities such as rest, splinting, heat, ice, physical therapy and non-steroidal anti-inflammatory medications. In severe cases, surgical decompression of the nerve may be necessary.

